

As of the 21st of April, Ireland has vaccinated nearly 905,000 people or 23.4% of the population with at least their first dose. Some countries are performing much better – Israel leads the world with 61% of the population inoculated while the UK trails second with just under 58%. Though our vaccine programme has been sluggish, the effects have been seen with last week being the first without a recorded death in those over 65 since the pandemic began. April is also set to be the month 1 million vaccines are to be delivered and distributed in Ireland, allowing us to progress from the 70+ cohort onto younger groups.
Ireland’s vaccine supply is sourced through the EU commission, which secures access and contracts to vaccinations on behalf of EU member states. So far, the commission has set up arrangements to procure 1.86 billion vaccines for the EU plus an additional 600m Sanofi-GSK and CureVac vaccines should they be approved. As a whole, rich nations which make up about 15% of the world’s population, possess about 53% of the world’s vaccines. The UK with a population of 66m people has purchased nearly 400m vaccines, with the dubious intention of “donating surplus vaccines to lower/middle income countries”.
French President Emmanuel Macron has also made similar overtures saying that France (and other EU member states) intends to donate “5% of their vaccine supply” to poorer countries. All in all, rich countries manage to vaccinate one person every second while most lower-income countries have not even begun their vaccination programmes. Currently, the EU expects the bulk of vaccination to be completed by mid-2021, China and India and other middle-income countries expect to be finishing at the end of 2022 while lower-income countries like Afghanistan and Bangladesh will not finish until the end of 2023 with 85 of these low-income countries not expecting to even begin vaccination before 2023.
Viruses, like COVID-19, exist to replicate themselves. They infect host cells (respiratory cells in humans) and alter those cells so that instead of producing their own proteins they produce the COVID-19 virus. Each time the virus creates a copy of itself, there is the potential for an error to occur which results in a slightly altered new copy of the virus that can have new properties. These errors could affect transmission (how the virus spreads) like the UK-variant which spread here during Christmas.
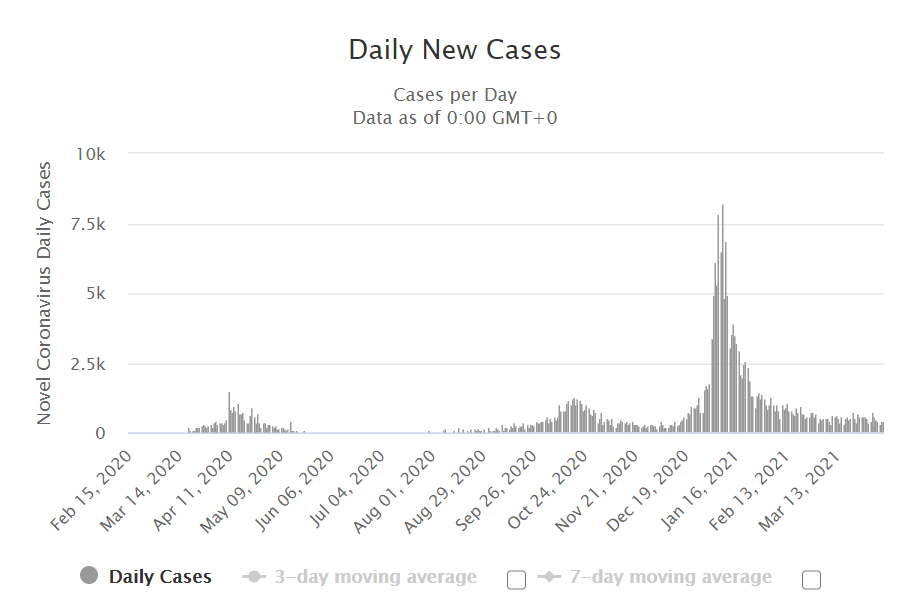
- Daily new cases in Ireland, third-wave spike beginning with easing of restrictions in December and importing of UK-variant to Ireland.
They could also affect the severity of the disease, making it more or less destructive to those infected. The South-African variant was rumoured to be associated with a more severe disease and possibly even resistance to vaccines.
The more a virus spreads the more mutated forms it produces. Vaccines work by exposing our immune system to some part of the COVID virion so that it recognises it and can produce antibodies (defence cells) against it. If the real COVID-19 is subsequently encountered, it’s quickly recognised, and the correct antibodies are produced. However, mutated forms of COVID could occur to which we’d have no protection. This really is a worst-case scenario, and the WHO expects vaccines to provide at least some protection to new variants, but they caution emphatically that we need to do whatever we can to stop the virus spreading anywhere so we can prevent it spreading everywhere. Their position is clear; none of us is safe until all of us are safe.
A collective effort needs to be made to supply lower/middle income countries with vaccinations. To this end the EU has set up COVAX; a scheme designed to provide 92 countries with the ability to access vaccines for up to 20% of their populations at a reduced rate, early projections expect that 1.2 million Pfizer doses and 336 million AstraZeneca doses will be delivered through this scheme to participating countries by the first half of 2021. So far Ghana and the Ivory Coast have received 500,000 – 600,000 each while Moldova and Bosnia and Herzegovina have received about 20,000. The doses from these facilities will initially go to healthcare workers than to those above 65 and those with co-morbidities.
The scale of this project is simply not large enough when compared to the EU’s vaccine stores which are on target to top 2 billion by the time most low-income countries will even be able to deliver a single dose. Even ignoring the dangers of allowing the virus to replicate and mutate explosively throughout most of the world, there are clear ethical and moral issues with vaccinating healthy cohorts that are not at any real risk from COVID while other countries cannot even vaccinate their most vulnerable or their health-care workers who assume the greatest risk in dealing with the virus.
James McDonnell, Science Contributor
